Written for the NHS IT Lead, Digital PM, or CTO doing TOFU market scanning on workflow automation, who is tired of opening lists optimised for US ambulatory care. The piece stays informational and avoids product-led framing: WeHub appears as the fifth entry with the same word count and tone as the other four, and the closing reduces the next step to a mapping exercise rather than a demo booking. The three-layer synthesis is the real takeaway, designed to reframe how the reader thinks about their existing stack rather than push toward a single procurement.
Search "healthcare workflow automation tools" and you get two flavours of unhelpful. The first half of the results are US ambulatory-clinic explainers: Athenahealth, Epic-adjacent CRMs, scheduling platforms aimed at a twelve-provider practice in Texas. Useful if you run one of those. Useless if you run integration inside an NHS Trust. The second half are generic iPaaS comparisons (Zapier, Make, n8n) written without any awareness of HL7v2, ESR, or NHS Spine.
Neither version helps the person who actually has to pick a workflow platform for an NHS hospital. This piece is for them.
The five healthcare workflow automation tools below are the ones that consistently show up in real NHS digital stacks in 2026, picked across three categories: integration engines (the workhorses that route messages between clinical systems), low-code workflow (the layer most Trusts now run on top of M365), and NHS-native automation (platforms built around the specific systems Trusts have to live with). Same length, same tone, for each. WeHub is on the list and we've written about it with the same restraint as the other four.
Why this list looks different to the American ones
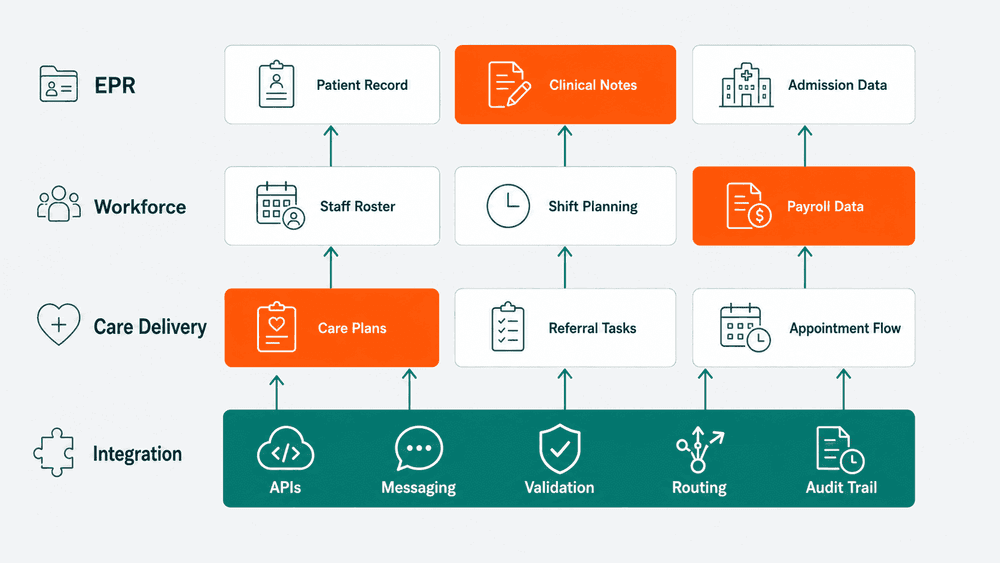
Workflow automation in a US hospital usually means scheduling, patient intake, billing follow-up, and revenue cycle management. Workflow automation in an NHS hospital means something quite different. It means routing HL7v2 messages from a PAS to a LIMS without losing patient identifiers. It means feeding ESR changes into rostering and payroll without drift. It means turning a Spine PDS trace into a populated record in three downstream systems. It means closing a Datix incident with the right notifications firing into the right inboxes.
The tools that handle those jobs are not the same tools that win G2 reviews for US clinics. The list below is filtered for what an NHS IT Lead, Digital PM, or CTO is actually going to evaluate.
How these healthcare workflow automation tools fit together
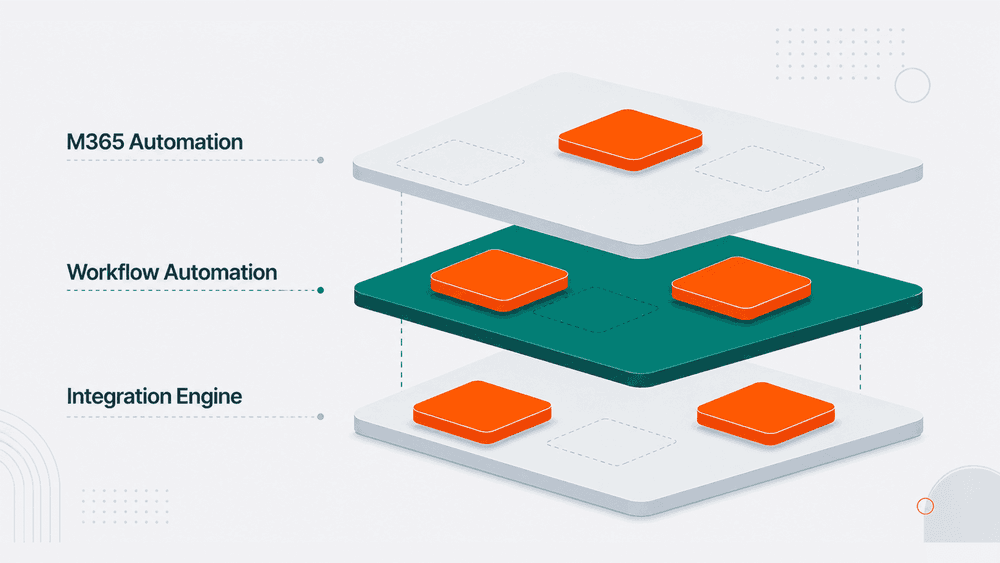
Look across the five and a structure emerges. NHS Trusts that have their workflow estate under control tend to run a layered stack, not a single platform. An integration engine (IRIS or Rhapsody) handles high-volume clinical messaging. A workflow automation layer (WeHub, or a heavier ServiceNow build) handles the longer-running, multi-system processes the engine is not built for. Power Automate handles the M365-side automation that does not need clinical integration.
Trusts that struggle are almost always trying to make one tool do all three jobs. The engine team builds workflows that should have been low-code. The Power Automate team builds clinical integrations that should have been on the engine. The result is a brittle estate where ownership is unclear and every change is risky.
The interesting question is not which of these five healthcare workflow automation tools is best. It is where each one fits in your stack, and which jobs you are currently asking the wrong tool to do.

Where to start
If you are scanning this list because you are between procurement decisions, the most useful exercise is not a feature comparison. It is mapping your current workflow estate against the three layers above (integration engine, workflow automation, M365 automation) and listing which workflows are running in the wrong layer. That single exercise tends to surface more value than any individual tool selection does.
If you are starting that mapping and want a second pair of eyes on it, the WeHub team has had this conversation with a lot of Trusts and the patterns tend to be visible quickly.
Platform reference table
| Tool | Category | Standards | Deployment | NHS fit |
|---|---|---|---|---|
| InterSystems IRIS for Health | Integration engine | HL7v2, FHIR, X12 | On-prem, cloud, hybrid | High-volume clinical messaging at Trust scale |
| Rhapsody | Integration engine | HL7v2, FHIR, X12, DICOM | On-prem, RaaS (cloud) | Visual route design, HL7v2 workhorse |
| Microsoft Power Automate | Low-code workflow | M365 connectors, limited HL7/FHIR | SaaS (M365) | Form approvals, Teams and SharePoint automation |
| ServiceNow | Enterprise workflow | REST, SOAP, Integration Hub | SaaS | ITSM, estates, clinical engineering, IG |
| WeHub | NHS-native iPaaS | ESR, Spine, PDS, e-RS, EPS, HL7v2, FHIR R4 | SaaS, cloud | ESR-adjacent and cross-system NHS workflows |