Auto-selected primary audience: Director of Finance / Deputy DoF and the Digital Programme Manager or IT Lead who writes the business case for them. BOFU positioning assumes the reader has accepted that automation works and is now justifying spend, so the piece is built around the finance objection rather than the technology. Search intent is INFORMATIONAL, so there's no CTA and no product pitch; the credibility of a BOFU finance-facing piece would be undermined by selling. The article gives the reader a defensible method they could apply with or without WeHub, which is exactly what earns the trust that converts later. Structure chosen: technical/architecture explainer pattern adapted to a financial-reasoning topic (problem framing, why it's hard, the working pattern, the bottom line).
A Director of Finance reads an automation business case and asks one question: "Where does the money come back, and when?" If the answer is a slide about efficiency and staff satisfaction, the case is already in trouble. Not because those things don't matter, but because they don't survive the scrutiny that a capital or revenue commitment gets in an NHS Trust running a tight position.
This is the gap most healthcare automation ROI cases fall into. The savings are real. The way they're counted is wrong. And the people building the case (often a Digital Programme Manager or an IT Lead who has watched a manual process consume their team for years) know the value is there but struggle to express it in the language finance actually signs off against.
This piece is for the person writing that business case. It's about where the return on healthcare automation genuinely lives in a Trust, which costs get quietly forgotten, and how to assemble a case that holds up when someone asks the hard version of the question.
The business case that doesn't survive contact with finance
You've seen the version that fails. It opens with hours saved. A process takes a band 4 forty minutes a day, automation takes it to five, the deck multiplies it out, and there's the headline: hundreds of hours a year recovered.
Then finance asks the question that ends the meeting. "So which posts are we removing?" And the honest answer is none, because those forty minutes were never a whole job. They were scattered across a role that's still needed for everything else. The hours are real but they don't convert to a cashable saving, and once that's clear the whole case loses credibility, including the parts that were genuinely strong.
The problem isn't the automation. It's that the case was built on the one form of return that finance trusts least: time, expressed as if time were money. In an NHS Trust, recovered time is real value, but it's almost never a line you can take out of a budget. Building the headline on it means the strongest argument collapses first.
Why healthcare automation ROI is harder to prove than it should be
Healthcare automation ROI is genuinely harder to demonstrate than ROI in most sectors, and it helps to be honest about why before trying to model it.
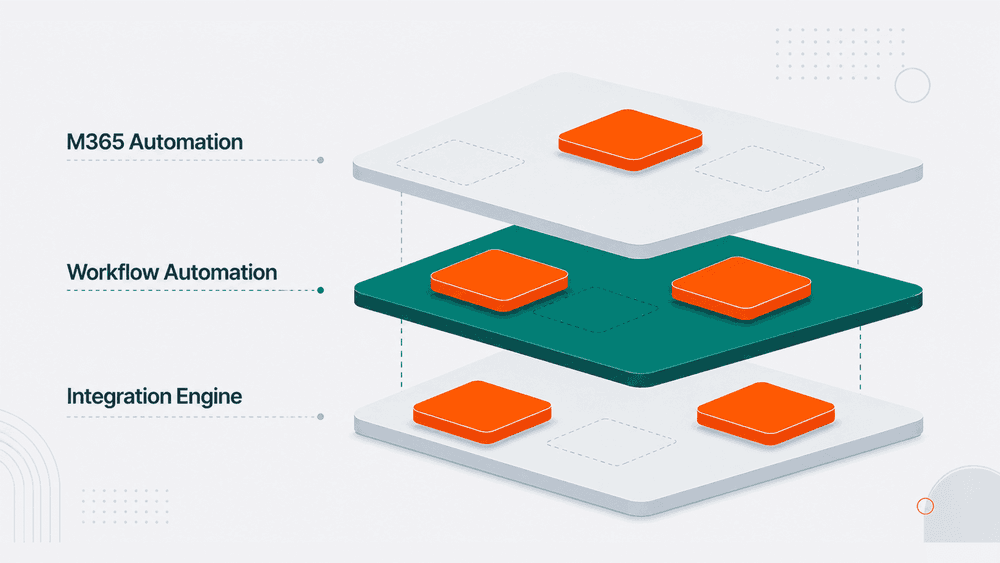
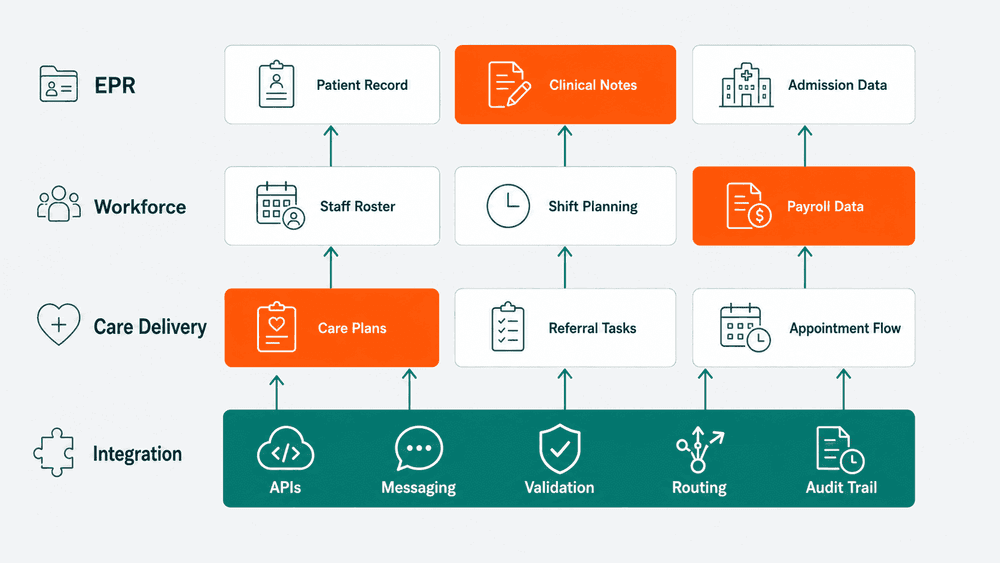
The return is distributed. A single automated workflow between ESR, rostering, and payroll might reduce overtime errors, cut the time a workforce team spends reconciling files, lower the risk of a payroll dispute, and improve the data feeding a BI dashboard. Four different benefits, owned by four different teams, landing in four different cost centres. No single budget holder sees the whole return, so no single budget holder champions it.
The biggest returns are also avoidance, not reduction. The strongest case for automating a Spine or PDS reconciliation isn't the hours saved. It's the duplicate record that never gets created, the data quality incident that never reaches the DSPT submission, the manual rekeying error that never becomes a patient safety report. Avoided cost is harder to put on a slide than reduced cost, but in healthcare it's usually the larger number.
And the baseline is often unknown. Trusts frequently can't say what the current process actually costs, because it's absorbed across roles, never measured, and treated as just how things are done. You can't prove a return against a baseline nobody has quantified. Half the work of an honest ROI case is establishing what the manual process costs today.
The four places the real return actually lives
When you stop leading with raw hours and look at where automation actually changes the Trust's position, the return tends to sit in four places.
1. Cashable cost, where it genuinely exists. Sometimes automation does remove a real cost: an agency spend driven by a slow manual process, a software licence made redundant, a recurring overtime line caused by month-end reconciliation crunch. This is the smallest category but the most credible, so where it's real, lead with it and evidence it precisely.
2. Capacity redirected to higher-value work. This is recovered time, but framed honestly. The band 6 who spent two days a month reconciling absence files now spends them on workforce planning the Trust couldn't otherwise resource. The value isn't a removed post, it's work that gets done that previously didn't. Finance will accept this when you name the specific work the capacity is redirected to, not when you express it as abstract hours.
3. Risk and avoided cost. The payroll dispute that doesn't happen. The IG incident that doesn't reach the ICO. The duplicate PDS record that never propagates downstream. Each carries a cost (investigation time, remediation, reputational and regulatory exposure) and automation that prevents the error prevents the cost. Quantify these as expected value: likelihood times cost, framed clearly as an estimate rather than a hard figure.
4. Decision quality from better data. When reconciliation runs continuously rather than monthly, leadership sees accurate workforce and activity data days earlier and acts on it. This is the hardest return to quantify and the easiest to overclaim, so treat it as a supporting benefit, not the headline.

The costs Trusts forget to count
An ROI case that only counts benefits gets discounted on sight. The credible ones count cost honestly, and these are the lines that routinely get missed.
Implementation is more than licence. Integration work, testing against a live ESR or Spine connection, information governance review, DSPT alignment, and the internal time of the people configuring and validating the workflow all count. A case that shows only the platform cost looks naive to anyone who has run a project.
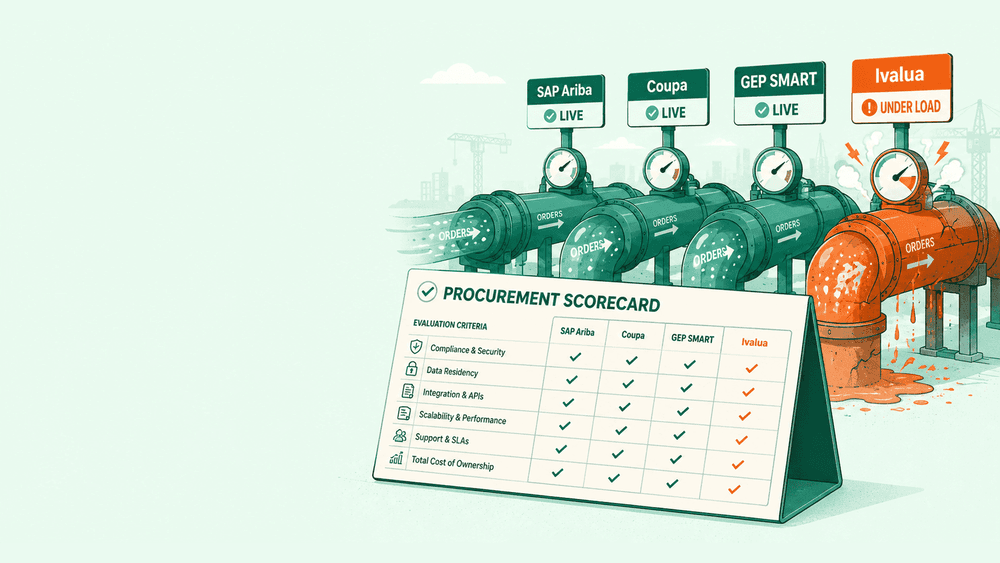
Then there's the cost of the integration itself behaving badly, which is the line almost nobody includes. An automated workflow that fails silently can cost more than the manual process it replaced, because a human checking a file notices when something looks wrong and an unmonitored pipe doesn't. The cost of monitoring, reconciliation, and exception handling is part of the real total, and including it makes the case stronger, not weaker, because it shows you've thought past go-live.
Finally, the do-nothing cost. The strongest ROI cases quantify the cost of the current manual process continuing: the error rate, the rework, the staff time, the risk exposure carried every month it stays manual. The comparison isn't automation versus zero. It's automation versus the real, ongoing cost of the status quo, and naming that cost is often what moves the decision.
How to build an ROI case finance will sign off
The pattern that works in a Trust is less about a clever model and more about counting the right things in the right order.
Start by measuring the baseline before you propose anything. Time the manual process, count the error rate, log how often the downstream dispute or incident actually happens. A week or two of honest measurement gives you a defensible number, and a defensible number is worth more than an impressive one.
Lead the case with cashable savings and avoided cost, the two categories finance trusts most. Put recovered capacity second and name the specific higher value work it enables. Treat better decision making as a supporting benefit, never the headline.
Count the full cost, including monitoring and exception handling, and show the do nothing cost alongside it so the comparison is honest. Then express the timeline plainly: when the Trust recovers the implementation cost, and what the position looks like in year two once the one-off costs are behind you.
A case built this way is harder to assemble than a slide of saved hours. It's also the one that survives the finance meeting, because every number in it answers the question that meeting always comes down to: where does the money come back, and when.
The bottom line
The return on healthcare workflow automation is real, but it rarely lives where the first draft of the business case puts it. It's in avoided cost more than reduced cost, in redirected capacity more than removed posts, and in the do nothing cost the Trust is already paying without counting it.
If you're building the case this quarter, start with one thing this week: measure the current process honestly before you propose the automation. The baseline is the hardest number to get and the one that makes every other number in your case credible. Get that, and the rest of the argument almost writes itself.