Written for senior NHS IT Leads, integration architects, supplier-side CTOs, and Digital Programme Managers who already know what FHIR, HL7v3, and ESR are and don't need them defined. The piece deliberately frames Spine as a delivery and assurance problem rather than a pure technology one, because that's where this audience has actual leverage. INFORMATIONAL/TECHNICAL_EXPLAINER intent: positioned for someone who is mid-scoping a Spine programme and wants the realistic shape of the work before they commit to a plan, which is why the closing reduces the next step to a single, manageable action rather than a generic CTA.
The kickoff meeting that always starts the same way
The kickoff meeting goes well. The clinical safety lead, the integration architect, the supplier engagement manager, and someone from procurement all agree on the goal: connect the new digital health product to NHS Spine so demographics, prescriptions, and referrals flow cleanly into the workflow.
Six weeks later, the same room. Smartcards still haven't been issued. The supplier's ASID lives in a spreadsheet someone else owns. The DCB 0129 evidence pack hasn't been started. The dev team has built against an endpoint that turns out to be wrong, and discovered the FHIR API they planned to use doesn't exist for the workflow they need.
This is the part nobody briefs you on at the start. The Spine build is rarely the long pole. The identity, assurance, and environment work around it is.
If you've delivered a Spine integration before, you already know. If you're approaching it for the first time as an NHS IT Lead, Digital Programme Manager, or supplier-side CTO, here's NHS Spine explained the way it actually behaves once a real project hits it.
What "connecting to NHS Spine"; actually means
NHS Spine isn't an API. It's a federation of national services run by NHS England (since the NHS Digital merger), each with its own purpose, identifier model, and integration pathway. Treating it as one system is the first place projects go wrong. Budgets and timelines get set against a single integration when the reality is six or seven of them, in different states of technical modernisation.
The services that matter for most digital health products sit under one Spine umbrella but behave like distinct platforms. They share an identity backbone and a directory, but the messaging patterns, the API generations, and the conformance gates differ across each one. A team writing a project plan needs to know which services the workflow actually touches before any estimate has meaning.
The Spine services you'll actually integrate with
Most builds only need a subset. Mapping the clinical or operational workflow to the specific services it depends on is the cheapest hour you'll spend on the project.
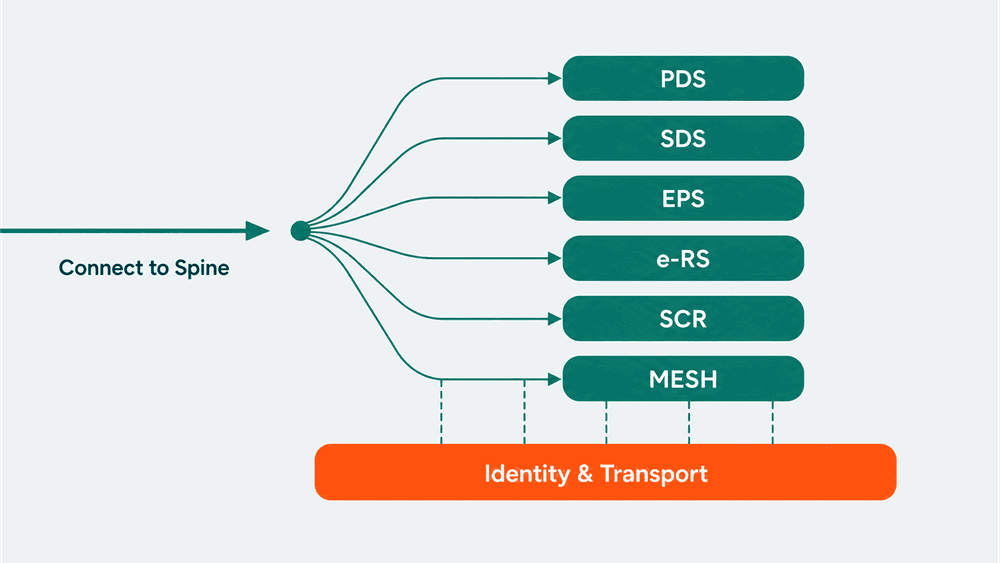
Personal Demographics Service (PDS). The national source of truth for patient demographics and NHS number tracing. Almost every patient-facing build touches PDS, either to verify identity at registration or to keep demographics fresh against the national record.
Spine Directory Service (SDS). The directory of every accredited system, organisation, endpoint, and certificate registered with Spine. SDS is what tells your message where to go and which system is allowed to receive it.
Electronic Prescription Service (EPS). Prescription lifecycle messaging between prescribers, dispensers, and the NHS Business Services Authority. EPS Release 2 is still partly HL7v3, with FHIR coverage growing.
e-Referral Service (e-RS). Outpatient referral booking and management. Typically integrated by primary care, referral management, and patient-facing booking products.
Summary Care Record (SCR). The national summary record, used most heavily in urgent and emergency settings. Read access is the common pattern; write access has tighter conformance.
MESH (Messaging Exchange for Social Care and Health). Secure file transfer between NHS organisations. Not an API in the modern sense, but a constant in workflows that move structured files between Trusts, GP systems, and national services.
There are others (SUS for secondary use data, Spine Mini Services for legacy lookups, NRLS for record locators), but the six above cover the majority of new digital health integrations.
The two integration eras: HL7v3 and FHIR
There are effectively two generations of Spine running in parallel.
The original Spine 2, built around HL7v3 messaging over the Transaction Messaging Service (TMS), with ebXML wrappers, and an MHS layer that resolves endpoints through SDS. This is the era where you'll meet party keys, interaction IDs, and asynchronous response patterns that don't look like anything you've integrated with elsewhere.
The newer NHS Digital API platform, exposing FHIR R4 over HTTPS with OAuth2 and JSON, sitting at api.service.nhs.uk. It now covers most read-side PDS lookups, increasing portions of EPS, parts of e-RS, and a steadily growing surface area.
The pragmatic position for a new build: design FHIR-first, and plan HL7v3 only where the workflow still mandates it. Some EPS prescription lifecycle events, certain PDS change notifications, and several inter-organisational flows still require the legacy stack. Assuming you can avoid HL7v3 entirely is one of the more common scoping errors.
A team that wires its architecture for both transports from the start, with a translation layer in the middle, is far better placed when the spec eventually catches up. A team that hard-codes against one transport learns this lesson the expensive way.

Identity, access, and the parts that block you
Three identity layers run through every Spine integration. Any one of them can stall delivery for weeks if it's not requested early.
User identity (CIS2). Care Identity Service 2 authenticates clinical users, historically through smartcards and increasingly through mobile credentials and OIDC-based flows. If your workflow involves a clinician acting on a patient record, CIS2 is in scope.
System identity (ASID and Party Key). Your software's identity to Spine. Issued by NHS England, registered in SDS, scoped to a specific environment, and tied to your organisation's ODS code. Each environment (INT, Path to Live, Production) has its own ASID.
Transport identity (mutual TLS and OAuth2). Certificates issued through NHS England's certificate authority, separate per environment, with rotation and renewal cycles to manage. The newer FHIR APIs lean on OAuth2 and signed JWTs alongside or instead of mTLS, depending on the API and the access mode.
None of these are issued instantly. Each has a request process, a turnaround measured in weeks rather than days, and prerequisites that often involve teams the supplier doesn't directly control. Starting these requests in week one, before any code has been written, is the highest-leverage decision a delivery lead makes.
Assurance: the part that takes longer than the build
The technical work to integrate with a single Spine API is rarely the bottleneck. The assurance work around it is.
DCB 0129 and DCB 0160. Clinical risk management standards. The supplier produces a DCB 0129 hazard log and clinical safety case for the product. The deploying organisation produces a DCB 0160 case for how it's being used in their environment. Both need a registered Clinical Safety Officer, and both need to be in place before live use.
DSP Toolkit (DSPT). Annual data security and protection submission. Required for every organisation handling NHS patient data. The connection between the supplier's DSPT, the deploying Trust's DSPT, and the data sharing agreement underneath them is what makes the integration legally defensible.
Connection assurance and conformance. Depending on the API, this might be a Target Operating Model assessment, a technical conformance test pack, a supplier conformance review, or a combination. The route differs by service and is documented per API on the NHS Digital developer site.
Penetration testing and security review. Standard for any production-bound integration handling patient data, with specific NHS expectations layered on top of generic best practice.
A realistic Spine programme runs assurance as a parallel track from day one, not as a final phase. The teams that defer it are the teams that miss go-live dates, every time.
The three environments, and why they matter
NHS Spine has three environments, and each one behaves differently.
INT (Integration) is the development sandbox. Synthetic data, looser gating, and the place to do the bulk of your build work.
Path to Live (still called Deployment, or Dep, in some places) is pre-production. Realistic message shapes, production-like configuration, and the environment where most genuine bugs surface. Skipping it, or treating it as a formality, is how teams discover at go-live that their FHIR client doesn't handle a particular response code, or that their HL7v3 acknowledgement timing is wrong.
Production is production. New ASIDs, new certificates, real patient data, and a much narrower window to fix anything that breaks.
Promotion between environments is gated, and each environment has its own ASID, its own certificates, and its own access requests. Plan for three of everything, not one.
How to plan a Spine integration that actually ships
The pattern that holds up across digital health builds is consistent.
- Map the workflow to specific Spine services first. "We need to connect to Spine" is not a scope statement. "We need PDS for demographics, EPS R2 for prescription send, and CIS2 for clinician auth" is.
- Default to FHIR APIs where they exist, and design the integration layer so HL7v3 fallbacks can be slotted in for workflows that still require them.
- Start ASID requests, smartcard provisioning, ODS code alignment, and certificate procurement in week one, before any code is written. These are the lead-time items that quietly determine your go-live date.
- Run DCB 0129, DCB 0160, and DSPT alignment as a parallel track from day one. Assign a named Clinical Safety Officer before the architecture is finalised, not after.
- Build against INT, validate against Path to Live, and assume Path to Live is where your real bugs will appear. Budget time accordingly.
- Treat reconciliation and observability as part of the build, not a post-go-live retrofit. Spine messages can fail in ways that look like success at the transport layer, and you want field-level logging in place before the first production transaction.
This is the pattern WeHub's workflow designer was built around, but the pattern itself matters more than any one tool. Any team running a serious Spine integration should be able to point to all six of these properties in their delivery plan.
Where to start this week
NHS Spine isn't difficult because it's poorly designed. It's difficult because it's a federation of services with overlapping identity layers, two API generations, and a mature assurance regime that exists for good reason. Treating it as one integration is what turns a six-month project into a twelve-month one.
If you're scoping a Spine programme right now, the highest-leverage thing you can do this week is map the workflow to specific Spine services and start the ASID, certificate, and CIS2 requests against that map. The build will catch up. The lead-time items, if you don't start them now, won't.