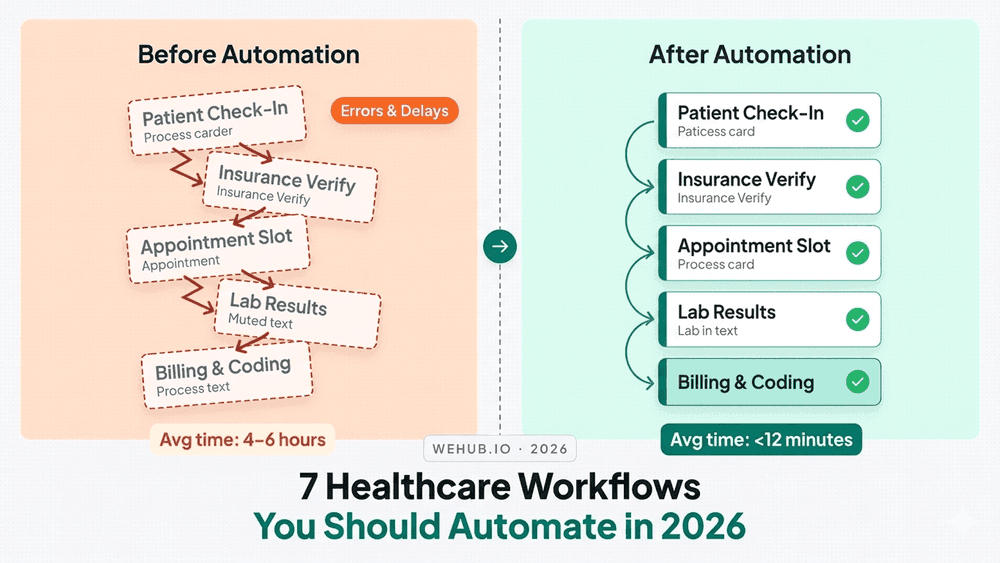
Manual workflows are one of the biggest hidden costs in healthcare operations. Here are seven that most digital health teams know are broken and what automating them actually looks like.
The automation gap hiding in plain sight
There's a meeting that happens in almost every NHS trust and digital health team at least once a quarter. Someone pulls up a spreadsheet. Someone else mentions that the same task has been done manually for years. A third person says they assumed it was already automated.
It wasn't.
Healthcare has made enormous strides in digitisation EPRs, patient portals, digital diagnostics but underneath those systems, a significant amount of operational work still runs on manual effort, spreadsheets, and staff goodwill. The automation gap isn't a technology problem. It's a prioritisation problem, and in 2026, it's becoming harder to justify.
Here are seven workflows where that gap is most costly and most fixable.
1. Referral Management and Triage Routing
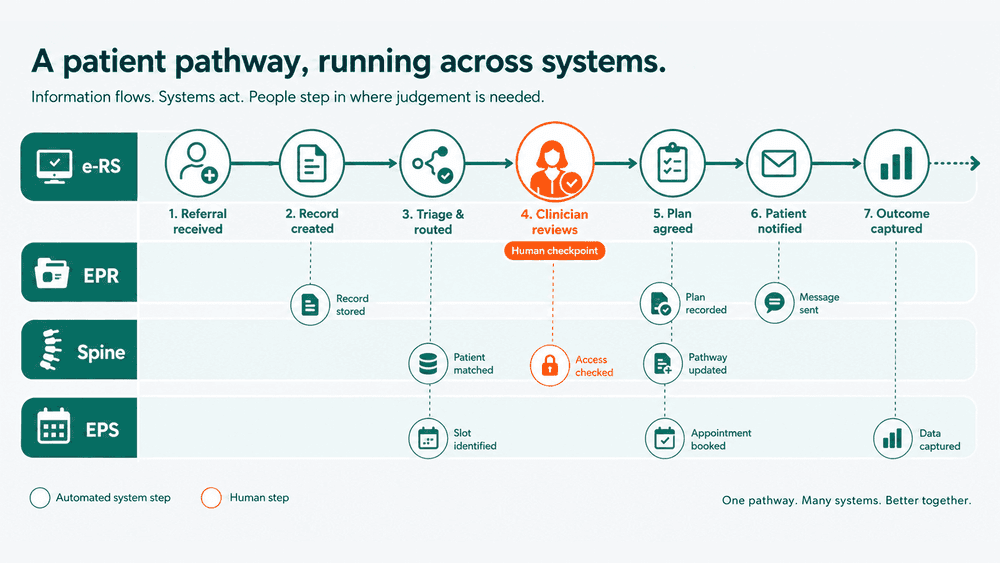
Referrals arrive through multiple channels: ERS, fax, email, GP letters, and sometimes phone calls. Each one needs to be logged, reviewed, triaged, and routed to the right team or clinician. In most organisations, that process involves at least one human touching the referral before it reaches the right inbox.
The cost is time. The risk is delay.
Automating referral intake validating against criteria, extracting key clinical data, routing based on urgency or specialty can reduce triage time significantly and create an auditable trail from receipt to action. The technology to do this exists. The integration work to make it happen is the real task.
2. Appointment Reminders and Patient Communication
DNA rates in the NHS average around 6–7%, but in some specialties and demographics they run higher. Most trusts know this. Many have reminder systems in place. Far fewer have those systems connected to their EPR in a way that adapts to cancellations, rescheduling, or patient preferences in real time.
The result: reminders go out for appointments that have already been cancelled. Patients who opted out of SMS still receive calls. Staff spend time managing exceptions that a well-configured automation would handle automatically.
This is one of the highest-ROI automation targets in outpatient operations. The logic isn't complex. The integration requirement a live connection to the scheduling system is where teams most often stop short.
3. Discharge Summary Generation and Distribution
Discharge summaries are clinically important, operationally painful, and chronically delayed. The GP needs them. The patient needs them. The system requires them. And in many trusts, they're still dictated, transcribed, reviewed, approved, and posted a chain of steps that can take days.
Automation here doesn't mean removing clinical judgement. It means pulling structured data from the EPR medications, diagnoses, procedures, follow-up actions into a pre-structured template that the clinician reviews and signs off, rather than writes from scratch.
The time saving per summary isn't enormous. Across a trust doing hundreds of discharges a week, it becomes significant quickly.
4. Clinical Document Ingestion and Filing
Documents arrive constantly: outpatient letters, test results, imaging reports, external referral responses. Many are still arriving as PDFs, faxes, or scanned images. Someone has to open them, identify the patient, attach them to the correct record, and file them under the right category.
This is low-skill, high-volume work that consumes staff time and creates risk when it falls behind. Automation OCR extraction, patient matching, rules-based filing can handle the majority of this volume with human review reserved for exceptions.
The challenge is patient matching. Ambiguous demographics, missing NHS numbers, and inconsistent naming conventions mean that automation needs to be tuned carefully, with a clear escalation path for anything it can't confidently resolve.
5. Staff Onboarding and System Access Provisioning
A new member of staff joins on Monday. By Wednesday, they still don't have access to the EPR. By Friday, someone from IT has sent three emails and a ticket has been raised.
This scenario is so common it's become background noise. But the cost is real in lost productivity, in clinical risk when staff use shared logins as a workaround, and in the administrative burden on HR and IT teams processing requests manually.
Automating the joiner workflow triggered by an ESR record status change, provisioning system access based on role and department, routing approval to the line manager is technically straightforward. The blockers are usually organisational: who owns the process, whose system triggers the automation, and how exceptions are handled when a role doesn't map cleanly to a permission set.
6. Results Notification and Follow-Up Flagging
Abnormal results need to reach the right clinician quickly. Normal results still need to be filed and acknowledged. In between those two states, there's a notification and routing process that in many organisations still relies on humans checking worklists, printing results, and chasing acknowledgements.
Automating results notification routing based on result type, flagging abnormal values above a threshold, confirming acknowledgement, escalating if no response within a defined window reduces the risk of results going unactioned and removes the administrative overhead of manual chasing.
This is one of the areas where the clinical stakes are highest. The automation needs to be reliable, auditable, and designed with clinicians, not just around them.
7. Reporting and Compliance Data Collection
Someone, somewhere in your organisation, spends hours every month pulling data from multiple systems, reconciling it, formatting it, and submitting it to a commissioner, regulator, or internal governance team.
This is almost always manual. It is almost never documented. And when the person who does it leaves, the knowledge walks out with them.
Automating data collection for performance reporting, CQC submissions, contractual KPIs, and DSPT evidence doesn't require building a data warehouse. It requires identifying the sources, agreeing the definitions, and building a scheduled extraction and formatting process that runs without someone initiating it manually.
The reduction in effort is meaningful. The reduction in risk of errors, of late submissions, of key-person dependency is more meaningful still.
Where to start
The honest answer is: start with the workflow your team complains about most.
That complaint is usually pointing at something that is high volume, low complexity, and manually handled only because no one has prioritised fixing it. Those are exactly the conditions that make automation tractable.
Pick one workflow from this list. Map what actually happens today every step, every system touched, every person involved. Then identify where the integration points are, what data needs to move, and what the exception cases look like.
Digital health workflow automation doesn't have to start with a platform selection or a six-month project. It starts with understanding one broken workflow well enough to improve it.