Written for the senior NHS IT Lead, Trust CTO, and integration architect who already understand HL7v2, FHIR, MLLP, and channel-based engine architecture and don't need any of those defined. The piece deliberately avoids replacing-the-engine framing. Most readers will have a Cloverleaf, Rhapsody, Mirth, Ensemble, or BizTalk estate that's stable and doing real work. The argument is structural mismatch, not vendor failure, which is why the closing recommends coexistence and incremental migration rather than a rip-and-replace. MOFU positioning: assumes the reader has felt the gap and is now thinking through what a workflow layer above the engine should look like. The single WeHub mention is contextual, not a CTA. The credibility of the architectural argument has to do the work.
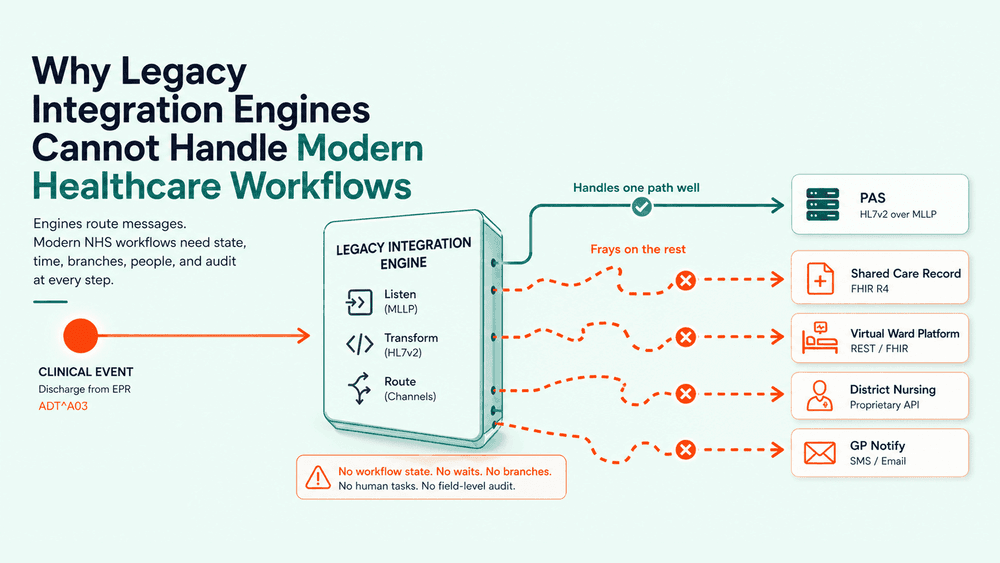
The request lands in the integration team's queue and looks routine on the surface. A discharge from the EPR needs to update PAS, push a FHIR Encounter to the Shared Care Record, enrol the patient on the community virtual ward platform, schedule a follow-up task in the district nursing system, and notify the GP. One clinical event. Five downstream consequences. Field-level audit required throughout.
The engine handles the first part without breaking a sweat. It picks up the ADT^A03, transforms it, and routes it to PAS over MLLP. That's what it was built for. Everything after that becomes bespoke. A TCL script here, a scheduled job there, a custom channel that does half a workflow and hands the other half to a human. Six weeks in, the team is still wiring it. Three months in, nobody can tell you what state any given discharge is in without running a SQL query against four different databases.
This is the pattern playing out in Trust integration teams across the country. The engine works. The workflow doesn't. And once you see it, you start to see legacy integration engine limitations everywhere, not just in clinical flows, but in every modern process that crosses more than two systems.
This piece is for the NHS IT Lead, Trust CTO, or senior integration architect who has done the channel-by-channel work for fifteen years and is now being asked for things the engine was never designed to deliver.
The integration request that exposes the gap
You can usually spot the request that breaks the model. It arrives with words like "trigger", "orchestrate", "wait for", or "update if". A virtual ward platform that needs the patient enrolled within an hour of discharge, but only if a community capacity check returns yes. A sepsis alert that needs to fan out to three systems, then wait for an acknowledgement, then escalate if it doesn't arrive. A PIFU pathway where the patient self-books a follow-up via NHS Login, the booking has to land in the EPR, and the clinic letter has to generate automatically.
None of these are message routing problems. They're workflow problems. They have state. They have time. They have branches. They have human approvals. And the engine in the middle of your Trust's integration estate has none of those concepts as first-class citizens. It has channels and transformations.
The mistake isn't that legacy engines were poorly built. They were built brilliantly, for the world they were built for: point-to-point HL7v2 messaging between PAS, EPR, lab, radiology, and pharmacy. The mistake is asking them to do something that's structurally different.
What legacy integration engines were actually built for
Strip the marketing off and a traditional integration engine is doing three things well. It's listening on a channel, usually MLLP, sometimes a file drop or a database polling job. It's transforming the message, usually HL7v2 to HL7v2, occasionally to a flat file or a SQL insert. And it's routing the result to one or more destinations.
That model worked because the workflows it served were synchronous, atomic, and stateless from the engine's point of view. An ADT^A01 came in, a transformation ran, a message went out. If the destination was down, the message queued. If the transformation failed, an exception fired. The engine didn't need to know what happened next, because what happened next wasn't its problem.
Modern NHS workflows broke that assumption. The engine is now expected to be an orchestrator of multi-step processes that span synchronous and asynchronous systems, internal and external, HL7v2 and FHIR R4 and REST, with human decisions in the middle and field-level audit at every step. That is not a configuration change. That is a different category of software.
What modern healthcare workflows actually require
Five characteristics show up in almost every workflow Trusts are now being asked to deliver:
State. The workflow has to know where any given instance is: enrolled, awaiting review, escalated, completed, cancelled. Channels don't carry state. They carry messages.
Time. The workflow has to wait. Wait for an acknowledgement. Wait for a clinical decision. Wait until 48 hours post-discharge to send a check-in. Engines can schedule, but they don't model time as part of a process.
Branching. The workflow has different paths depending on data, capacity, consent, or human input. A transformation can branch on field values. A workflow has to branch on outcomes from other systems.
Human-in-the-loop. Someone has to approve, review, or triage. The workflow needs to present that decision, capture the response, and continue. Engines have no concept of a task queue.
Observability at the workflow level, not the message level. When something goes wrong, the question is "what happened to this referral?", not "did the message route successfully?". Channel-level monitoring tells you the second. It cannot answer the first.
If you map these five against your current integration estate, the gap becomes obvious. Most legacy engines have partial answers to one or two of them, achieved by wrapping bespoke code around the channel layer. None have all five as native concepts.
Six places legacy engines fail in modern workflows
These are the failure modes that show up most often in Trust integration projects once the workflow ambition outgrows the engine.
1. No native workflow state.
The engine routes a message and forgets it existed. To track a multi-step workflow, teams build a sidecar database, write status updates from inside transformation scripts, and pray nobody bypasses the channel. Six months in, the sidecar is the source of truth and the engine is just a router. You've built a workflow platform around the engine, not with it.
2. Synchronous mindset in an asynchronous world.
Modern workflows wait. For a clinician to acknowledge. For a patient to respond to an SMS. For a partner Trust to confirm capacity. Legacy engines treat waiting as failure: a timeout, a retry, an exception. Modelling a 48-hour wait as a process state, not an error condition, is something they fundamentally don't do.
3. FHIR is bolted on, not native.
Most legacy engines added FHIR support as a transform target. The data model underneath is still the engine's internal HL7v2-shaped representation. When you need to reason about a FHIR Bundle, link a Condition to an Encounter to a Practitioner, or post to a partner FHIR server with OAuth2 and SMART on FHIR scopes, the gap shows. Modern healthcare integration tools were built FHIR-first. The engine wasn't.
4. Modern auth is a configuration battle.
NHS Login. CIS2. OAuth2 with refresh tokens. mTLS to Spine. Each takes hours of bespoke configuration in most legacy engines, often with custom Java or scripted hacks for token refresh. The engines that handle this cleanly were rebuilt around it. The ones that didn't expose the seams every time a token expires.
5. Field-level audit doesn't exist by default.
DCB 0129/0160 and DSPT both increasingly want to see what happened to a piece of data: what came in, what was transformed, what was written, by whom, when. Most engines log at the channel level: message received, message processed, message sent. Reconstructing what changed inside the transformation, for a specific patient, in response to an IG query, is a forensics exercise rather than a query.
6. Deployment and change control don't fit modern delivery.
Channels live as configuration in a single engine instance. Promoting a change from test to live often means manual export-import, with no real version control, no diff, no rollback strategy beyond "restore from backup." Trusts trying to run integration on a CI/CD model, with reviewable changes, environment parity, and traceable releases, find the engine is the part of their stack that resists modern delivery hardest.
Each of these can be worked around. None of them stop being friction. Cumulatively, they're the reason a "simple" integration that should take two weeks takes three months.
From message routing to workflow orchestration
The architectural shift the rest of the industry has already made, and that NHS Trusts are now navigating, is from message routing to workflow orchestration. The two patterns sit at different levels of abstraction.
A message router thinks in channels. Each channel is a pipe with a transformation inside it. The unit of work is a message.
A workflow orchestrator thinks in processes. Each process is a definition with steps, state, branches, waits, and outcomes. The unit of work is a workflow instance, which may consume and emit many messages across its lifetime.
The orchestrator does not replace HL7v2 routing. Trusts still need MLLP listeners, ADT processing, lab feeds. What changes is that those routing operations become steps inside larger workflows, rather than being the workflows themselves. The engine becomes one tool inside a broader integration platform: useful, but no longer load-bearing for processes it was never designed to carry.
This is the pattern modern healthcare integration tools are built around. WeHub's workflow designer treats the workflow as the primary artefact, with HL7v2, FHIR, REST, file transfer, and human tasks as steps inside it. The engine model treats the channel as the primary artefact, with everything else hanging off it. Both views can be valid for different problems. Only one of them scales to the workflows Trusts are now being asked to build.

What this means for Trust IT leads
Replacing a legacy engine wholesale is rarely the right first move. The engine is doing real work on stable HL7v2 flows that don't need to change. The risk isn't the engine itself. It's continuing to extend it into territory it doesn't fit.
Three practical moves that consistently work:
Identify the workflows that have outgrown the engine. The signs are clear: bespoke sidecar databases, scheduled scripts that nobody documents, channels that have grown into 800-line transformation files, integrations that take a quarter to ship. Those are the workflows that need orchestration, not more channels.
Run the orchestrator alongside the engine. The orchestrator handles the new workflows and calls into the engine where HL7v2 routing is still the right answer. Over eighteen to twenty-four months, the engine's footprint shrinks naturally as workflows migrate. Nothing has to be replaced under deadline pressure.
Make field-level audit and workflow-level observability non-negotiable in the new layer. This is where DSPT, DCB 0129/0160, and IG conversations either become routine or become painful. Choose the tooling that makes them routine.
The bottom line
Legacy integration engine limitations are not a failing of the products. They're a category mismatch. The engines were built for a world of point-to-point HL7v2 messaging that still exists and still matters. They were not built for stateful, asynchronous, branching, auditable, human-in-the-loop workflows, and no amount of bespoke scripting around the channel layer makes them into that.
If your team is being asked for workflows the engine cannot natively model, the question isn't how to extend the engine further. It's where the orchestration layer above it should live, and which of your current integrations should be the first to move. Pick one workflow that's currently held together with sidecar scripts and bespoke channels. Rebuild it as a real workflow with state, branches, and field-level audit. The same pattern, once it works for one process, is the one you'll reuse for every cross-system flow your Trust runs from here on.