Beyond the Hype: 5 AI Agents Quietly Reshaping Healthcare Operations
There's a meeting that happens every quarter in most NHS digital teams. Someone presents a slide about AI. The room nods. Then everyone goes back to fixing ESR extracts that broke on Tuesday and chasing down why a PDS trace is returning stale demographics for a subset of patients. The gap between the AI conversation and the operational reality isn't closing - it's widening.
But here's the thing: a handful of AI agents in healthcare are actually starting to earn their place. Not the ones promising to 'revolutionise care delivery' in a pitch deck, but the ones quietly reducing the manual work that keeps operational teams running two steps behind.
This isn't a vendor shortlist. It's a look at five categories of AI agents that are changing how healthcare operations actually work - and what you need to evaluate before bringing any of them into your environment.
What makes an AI agent different from a chatbot or a rule engine?
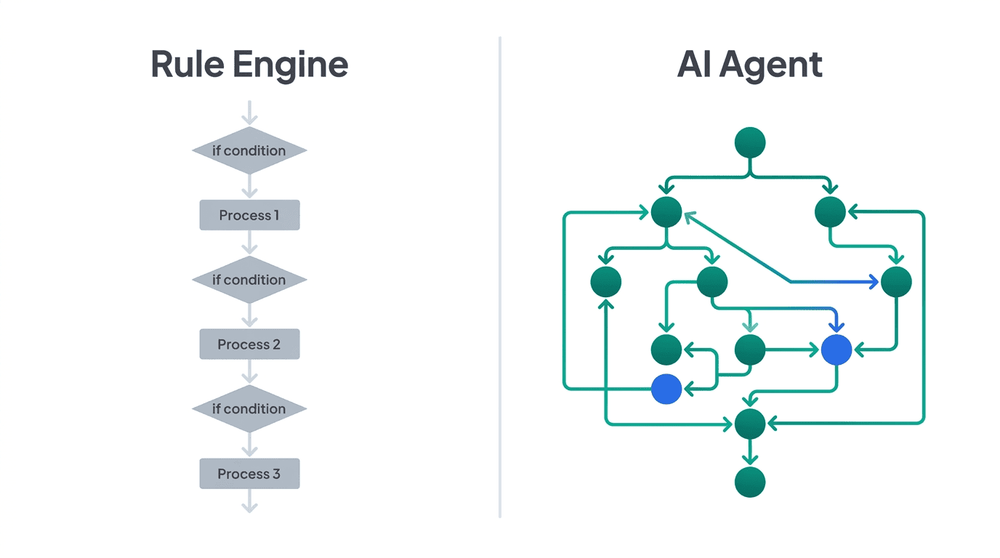
Worth clarifying, because the term gets stretched until it means nothing. An AI agent isn't a chatbot with better marketing. It's software that can perceive a situation, make a decision, and take an action - often across multiple systems - without a human triggering every step.
A rule engine fires when a condition is met. An AI agent decides which conditions matter. That distinction is what makes AI healthcare automation tools operationally interesting - and operationally risky, if governance isn't tight.
For NHS digital leads evaluating these tools, the question isn't "does it use AI?" It's: what decisions is it making, what data is it touching, and who's accountable when it gets one wrong?
Agent 1: Ambient Clinical Documentation
What they fix: Clinicians spend a significant chunk of their day on documentation. Ambient documentation agents - like Nuance DAX Copilot or Abridge - sit in the background during consultations, capture the conversation, and generate structured clinical notes in near real-time.
Why it matters operationally: This isn't just about saving clinicians' time, though it does. It's about what happens downstream. Better-structured notes mean cleaner coding, fewer queries from clinical coders, and reduced risk of incomplete records surfacing during audits. For NHS Trusts running EPR systems alongside legacy PAS configurations, the data quality uplift alone changes the workload profile for informatics teams.
What to evaluate: Integration depth. Can it write back to your EPR natively, or are you standing up another middleware layer? And critically - how does it handle consent, recording governance, and GDPR obligations in a multi-clinician, multi-room environment?
Agent 2: Referral Triage and Routing
What they fix: e-RS worklists that pile up. Referrals sitting in queues because triage is manual, inconsistent, and dependent on whoever happens to be working that day. AI triage agents - the kind being piloted across several NHS regions - read the referral content, assess urgency and appropriateness, and route to the right clinical pathway.
Why it matters operationally: The visible problem is long waits. The hidden cost is rejected or redirected referrals that consume clinical admin time, create patient frustration, and generate repeat work. A well-tuned triage agent doesn't just speed things up - it reduces the rework loop that clogs capacity planning.
What to evaluate: Training data provenance. If the model was trained on referral patterns from a different health system, its triage logic may not map to your Trust's pathway configuration. Also: does it explain its reasoning? If a clinician can't understand why a referral was routed a particular way, you've got a governance problem, not a productivity gain.
Agent 3: Workforce and Rostering Optimisation
What they fix: The spreadsheet-and-email choreography behind staff rostering. AI workforce agents - used by platforms building on ESR data feeds - can forecast demand, flag rota gaps before they become crises, and optimise shift patterns against multiple constraints simultaneously: skills, contracts, working time directives, and cost.
Why it matters operationally: Workforce is the single largest cost line in any NHS Trust, and rostering is where the inefficiency compounds. One unfilled shift cascades into agency spend, overtime, and staff burnout. The top healthcare AI agents in this space aren't replacing roster managers - they're giving them a three-day head start on problems that currently surface at 6am on a Monday.
What to evaluate: How cleanly it integrates with ESR. If the agent can't consume real-time ESR data - assignments, competencies, leave balances - it's working from a stale picture. And stale workforce data doesn't just reduce accuracy; it erodes trust with the nursing and operational teams who have to live with the output.

Agent 4: Revenue Cycle and Coding Agents
What they fix: Clinical coding backlogs and billing accuracy. AI coding agents review clinical notes, suggest appropriate codes, and flag discrepancies between documented care and submitted coding. In the NHS context, this maps to Payment by Results accuracy and national clinical coding standards.
Why it matters operationally: Coding errors aren't just a finance problem. They distort activity data, which distorts commissioning intelligence, which distorts resource allocation. An AI agent that improves first-pass coding accuracy by even a few percentage points changes the quality of data that flows into planning, benchmarking, and CQC reporting.
What to evaluate: Specificity of the model. Generic coding agents trained on US billing data (ICD-10-CM, CPT) won't map cleanly to NHS coding requirements (ICD-10 5th edition, OPCS-4). Ask where the training data comes from. If the vendor can't answer that clearly, walk away.
Agent 5: Integration and Workflow Orchestration Agents
What they fix: The brittle, manually maintained integration layer that connects your clinical, workforce, and administrative systems. AI workflow agents healthcare teams are starting to evaluate can monitor data flows, detect anomalies, auto-remediate common failures, and intelligently route exceptions across HL7 v2, FHIR, and flat-file interfaces.
Why it matters operationally: Integration teams spend a disproportionate amount of time on incident response - a failed Spine connection, an ESR extract that didn't run, or a PDS mismatch that's blocking patient merges. The compounding effect of these micro-failures is invisible to leadership but felt acutely by the digital teams absorbing them daily. An orchestration agent that can detect, diagnose, and in some cases resolve these issues before they become tickets shifts the team from reactive to strategic.
What to evaluate: Governance and audit trails. If an agent auto-remediates a data flow - say, retrying a failed HL7 message or requeuing an EPS prescription - there must be a clear, queryable record of what it did and why. In an IG-regulated environment, "the AI fixed it" isn't an acceptable audit response.
What connects these five
The pattern across all five of these AI agents in healthcare isn't intelligence for its own sake. It's the removal of predictable, repetitive operational friction - the kind that eats capacity without ever appearing on a board report.
Each of these agents works best when it's tightly integrated into the systems and workflows that already exist. None of them deliver value as a standalone product bolted onto the side. The NHS Trusts seeing genuine results are the ones treating AI agents as a layer inside their integration architecture - not a separate initiative with its own project board and twelve-month discovery phase.

The decision you're actually making
This isn't a decision about whether AI agents belong in healthcare operations. They're already there. The decision is whether your team evaluates them with operational rigour or gets sold something that looks good in a demo and quietly becomes another system nobody maintains.
Start with one problem. A specific queue that's always backed up. A data flow that breaks every month. A manual process that three people know how to do and none of them want to keep doing. Find the AI agent that addresses that exact friction point, evaluate it against your integration architecture and IG requirements, and run a controlled pilot.
That's not a twelve-month strategy. It's a decision you can make this month.