Healthcare interoperability is the ability of different systems to exchange data and actually use it. Not just transport it. Not just store it. Use it, in a real clinical or operational workflow, without someone re-keying it or chasing it through an inbox. In the NHS, that means getting HL7 v2 messages, ESR extracts, FHIR resources, and flat files to flow between PAS, EPR, workforce, and referral systems in a way that's structured, governed, and auditable. Most NHS digital teams sit somewhere between structural and semantic interoperability. The gap to organisational interoperability, where data flows across trust boundaries with proper governance, is where the real complexity lives. This guide covers the four layers where interoperability breaks, the standards you're working with (FHIR UK Core, HL7 v2, SNOMED CT, NHS Spine), the practical challenges no one warns you about, and how to start improving it without commissioning a twelve-month architecture programme. Pick one workflow, define one data contract, validate before you publish downstream, and measure one outcome that matters.
The Meeting That Happens in Every NHS Organisation
There's a meeting that happens in almost every healthcare organisation at some point.
Someone says the systems are already "connected." Someone else points out that staff are still copying information from one screen to another, patients are still being asked for details the service already has, and key updates still arrive late, incomplete, or in the wrong format. On paper, the data moves. In practice, the workflow still breaks.
That gap is where healthcare interoperability stops being an abstract technical term and starts becoming an operational problem.
if you're looking for healthcare interoperability explained in plain English: it's about making sure different systems can share information in a way that is actually usable, reliable, and safe in real healthcare work. Not just technically connected. Operationally useful.
Interoperability Is Not "Can We Send a File?"
The definition matters more than people think. Healthcare interoperability explained in the most practical way possible is this: the right data reaches the right place, in the right format, with the right meaning, in time for someone or something to act on it.
That means three things need to work together. Data can move between systems securely. The receiving system can understand the structure of that data. And the receiving team or workflow can use that data without manual cleanup or guesswork.
If any of those breaks, you don't have interoperability. You have transport. And transport is what most NHS organisations actually have today: data moves, but someone still has to open a PDF, retype a field, correct a code, or decide which record it belongs to. The work hasn't disappeared. It's just moved.
Poor interoperability rarely shows up as one dramatic failure. More often, it becomes background noise that everyone has normalised: a referral that needs manual checking because data arrived inconsistently, discharge information that exists but not where the next team needs it, workforce onboarding delayed by duplicate data entry, service managers trying to improve performance without confidence in the underlying data. The visible issue is usually delay or frustration. The hidden cost is much wider: staff time, operational fragility, patient confusion, governance risk, and lost trust in digital systems.
The Four Layers Where It Breaks
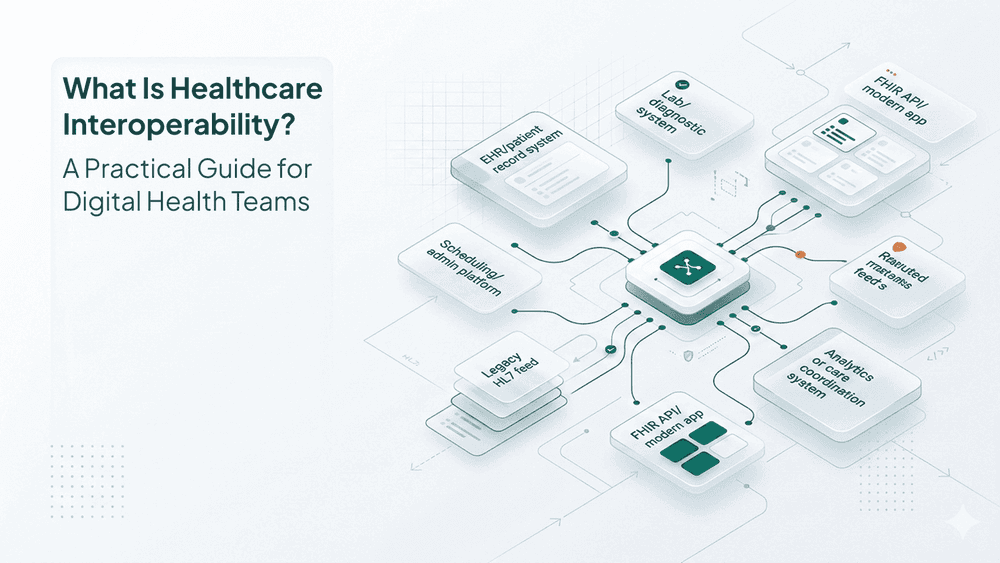
Most interoperability problems sit in one of four layers. Understanding which layer you're stuck at changes what you do about it.
- Technical interoperability. Can the systems talk at all? This is the transport layer: API access, secure messaging, file transfer, network routes, authentication. If you're still waiting for HSCN connectivity or a vendor to open an API endpoint, nothing else matters yet. Necessary, but not sufficient.
- Structural interoperability. Does the receiving system know what it received? A payload arrives. But is the date in the expected format? Are demographics in consistent fields? HL7 v2 messages, despite being a "standard," are implemented differently across trusts and vendors. What one system sends as a patient identifier another expects in a completely different segment. You discover this at 3am during a go-live.
- Semantic interoperability. Do both sides mean the same thing by the data they're exchanging? One system sends a status of "active." Another uses "current." One trust records department codes with ODS prefixes, another uses local naming. Without shared terminology (SNOMED CT, dm+d, ICD-10) and proper concept mapping, clean transport still produces messy outcomes. This is one of the most expensive failure points because it often surfaces late and requires costly rework.
- Operational interoperability. This is the part that gets ignored most often. Does the exchanged information arrive at the right point in the workflow, with the right context, permissions, timing, and traceability? Does it help a person do the next task with less friction? Operational interoperability is what people actually experience. It's the difference between a theoretically connected estate and a service that runs better. In the NHS, this is the layer where most projects stall.

The Standards Landscape You're Working With
You don't need every team member to become a standards specialist. But you need a shared understanding of what you're building on.
FHIR (Fast Healthcare Interoperability Resources) is where almost everything new is heading. RESTful APIs, JSON payloads, well-defined resources. NHS England's API and integration catalogue is built around FHIR, and FHIR UK Core is the baseline for anything being built for the English NHS. If you're starting a new integration from scratch, FHIR is the right starting point. Platforms like Microsoft Azure Health Data Services, Google Cloud Healthcare API, and healthcare-specific integration tools like WeHub all provide FHIR connectivity.
HL7 v2 is still everywhere in operational NHS environments. ADT messages, lab orders, referrals, discharge notifications. It works, it's deeply embedded, and it's not going away quickly. But implementations vary considerably between trusts and vendors, and it wasn't built for real-time APIs. Many NHS digital teams are managing HL7 v2 today while planning a FHIR migration for tomorrow. Integration engines like Rhapsody, InterSystems HealthShare, and WeHub handle both, which matters when you're bridging legacy and modern systems in the same workflow.
SNOMED CT is the clinical terminology standard, mandatory across NHS primary care. It ensures clinical concepts mean the same thing across systems. Without it, semantic interoperability is impossible. Getting terminology mapping right is one of the most underestimated parts of any integration project.
NHS Spine underpins the most critical national NHS services: PDS (Patient Demographics Service), EPS (Electronic Prescription Service), ERS (e-Referral Service), and more. If your application touches patient identity or national service workflows, you're integrating with Spine.
The important point is not to worship any single standard. FHIR doesn't magically create interoperability on its own. HL7 v2 isn't a failure just because it's older. Standards reduce ambiguity; they don't remove it. Teams still need mapping logic, validation rules, governance decisions, exception handling, and a clear view of who owns data quality.
Where It Actually Gets Stuck
Understanding what healthcare interoperability is and actually implementing it are different things. Here's where teams consistently run into difficulty
They connect systems, but not the process around them. A team integrates two platforms and considers the job done. Then they discover the handoff still needs a person to validate, reformat, or manually trigger the next step. The systems are connected. The service is not. ESR workforce data still arrives at most trusts as a nightly CSV drop via SFTP that has to be parsed, validated, and transformed before anything downstream can use it. That single data flow touches all four interoperability layers at once.
They underestimate local variation. The NHS is full of local realities: different providers, different operational models, different data quality, different naming conventions, different stages of digital maturity. A design that looks tidy in a diagram can behave very differently across real services. This is where centralised integration platforms (Power Automate, Workato, Tray.io, WeHub, and others) earn their keep: one place to manage, monitor, and govern data flows rather than maintaining dozens of bespoke point-to-point connections.
They treat standards as magic. FHIR helps. HL7 v2 still matters. SNOMED CT matters. But standards reduce ambiguity; they don't remove it. Teams still need mapping logic, validation rules, exception handling, and someone who owns data quality.
They validate too late. Bad data is cheapest to fix at the edge. Once incomplete, duplicated, or mismatched data has already spread across downstream systems, every correction costs more and takes longer. The strongest integration architectures validate before publishing, quarantine exceptions, and notify an owner.
They ignore governance until it's urgent. Even when systems are technically capable of sharing data, the legal and governance frameworks for doing so across NHS organisations are complex. DSAs, DPIAs, DSPT compliance, data controller agreements, Caldicott Principles. If the data moves but you can't explain who accessed it, why it moved, or whether it was shared appropriately, the design is incomplete. This is the layer where interoperability becomes an organisational challenge, not just a technical one.
They leave clinical and operational staff out of the conversation. Interoperability projects fail as often for organisational reasons as for technical ones. Workflows have to change. Staff need training. Vendors need to cooperate. Product teams, service managers, IG leads, and operational owners need to be involved early, because many failures are caused by assumptions about process, not just by technology.
What Good Interoperability Looks Like in Practice
When healthcare interoperability is working well, it becomes invisible. Clinicians have the information they need when they need it. Patients don't repeat themselves. Data flows without manual intervention. Audit trails are clean. Errors get caught early. Good interoperability usually feels boring. That's a compliment.
Take a referral workflow. A referral enters via e-Referral Service. Patient demographics are checked against PDS. Required fields are validated. The message is transformed into the structure your downstream system expects. The right patient record is matched. The right service line is identified. A triage task is created. The receiving team is notified. The outcome is logged.
No one downloads a CSV to inspect it manually. No one copies details from one screen into another. No one asks in a side channel whether the latest information lives in the EPR, the booking platform, or the inbox.
Or take workforce data. ESR extracts arrive daily via SFTP. They're parsed, validated against schema, transformed, mapped to the LMS's expected format, and published via API. Failed records are quarantined, not silently dropped. The L&D team sees new starters in their training system the same day, not next week.
That's what good interoperability in healthcare systems looks like. Not glamorous. Dependable. Information captured once and reused appropriately. Handoffs that happen without staff needing to chase context. Operational teams trusting the workflow enough to stop inventing side processes.

How to Start Without a 12-Month Programme
The biggest mistake digital teams make is treating interoperability as a giant transformation programme from day one. The teams that make progress usually do something smaller and much more disciplined.
Pick one workflow with visible pain. Start where data crosses systems and manual effort is already obvious: referrals, intake, discharge summaries, appointment updates, patient communications, test-result routing, staff onboarding. Pick one.
Map the real workflow, not the idealised one. Document what actually happens today. Include the spreadsheets, inboxes, manual checks, and handoffs people are embarrassed to admit are part of the process. That's the workflow you need to improve.
Define one stable data contract. Agree what data is required, what format it will use, which fields are mandatory, how errors are handled, and who owns changes. This is where interoperability becomes governable instead of tribal knowledge.
Validate before publishing downstream. Don't let bad data travel. Check structure, required fields, code values, and matching logic early. Quarantine exceptions. Notify an owner. Make failure visible.
Add monitoring and traceability from day one. If the workflow fails, you should be able to answer three questions quickly: what happened, where it failed, and who needs to act. If that takes an engineer, a shared inbox, and two meetings, the workflow isn't finished.
Measure one outcome that matters. Time saved. Error reduction. Faster turnaround. Fewer manual touches. Pick one metric before you go live. Otherwise, you'll end up debating whether the integration "feels better" instead of proving it works.
One workflow. One contract. One measurable outcome. That's usually how digital health interoperability stops being a strategy slide and becomes an operational improvement.

The Decision You're Actually Making
When teams discuss interoperability, the conversation can drift into standards, vendors, interfaces, and technical diagrams. Those matter. But the real decision is simpler than it sounds.
You're deciding whether important healthcare workflows will be held together by design or by habit
Habit looks like staff compensating for missing links, service managers carrying hidden risk, and clinical or admin teams doing quiet repair work every day. Design looks like information moving with enough structure, meaning, and governance to support the service properly.
If your systems can exchange data but your people still have to clean it up, chase it, reinterpret it, or prove what happened after the fact, the interoperability problem isn't solved yet. The organisations making the most progress in the NHS are treating interoperability as a product discipline, not just an IT project. They're starting with one workflow, one data contract, and one measurable outcome. And they're using platforms that handle the hard parts (parsing, validation, transformation, monitoring, governance) so their teams can focus on the clinical and operational problems that matter.
Don't begin by asking, "How interoperable are our systems?" Ask, "Which workflow still depends on people stitching the gaps together?" Choose one. Map it honestly. That's your starting point.
If your team is working through any of these challenges, we're happy to talk through what we're seeing across the NHS and where integration infrastructure like WeHub can make the most difference.