Written for senior NHS IT Leads, Digital Leads, and CTOs whose platforms integrate with NHS systems at scale. Assumes operational familiarity with Spine, PDS, ESR, e-RS, FHIR R4, HL7v2, MESH, SCAL, and DCB 0129/0160. The piece is deliberately pitched at the architecture layer rather than the introductory layer, because the reader already knows healthcare API integration is hard. MOFU positioning: assumes the reader is now evaluating which patterns to commit to and reduces the next step to one inventory exercise plus one reconciliation job rather than a generic discovery call.
The integration that looked done until it wasn't
Six months into a digital health platform's NHS rollout, the integration team is in a war room. The patient demographics on a referral don't match the Trust EPR. The SCR wasn't checked before the last batch went out. The Spine TLS certificate that nobody thought about expires in eleven days. The platform passed its SCAL submission cleanly. The FHIR endpoints work. The integration tests are green. And yet every one of those failures is happening in production.
This is the gap most healthcare API integration projects fall into. The technical pieces look fine in isolation. The system as a whole behaves nothing like a typical SaaS integration project, because the NHS isn't a typical environment, and treating it like one is the most expensive mistake a digital health team can make.
This piece is for the IT Lead, Digital Lead, or CTO whose platform talks to NHS systems at any meaningful scale, and who needs an architecture that survives audit, scale, and the ordinary chaos of Trust operations.
Healthcare API integration is not the API integration you trained on
Most engineers learn API integration on payment APIs, social platforms, or cloud SaaS. The mental model is consistent: synchronous REST, JSON in, JSON out, stateless, retry on 5xx, idempotency keys, OAuth, done.
Almost none of those assumptions transfer cleanly to NHS integration.
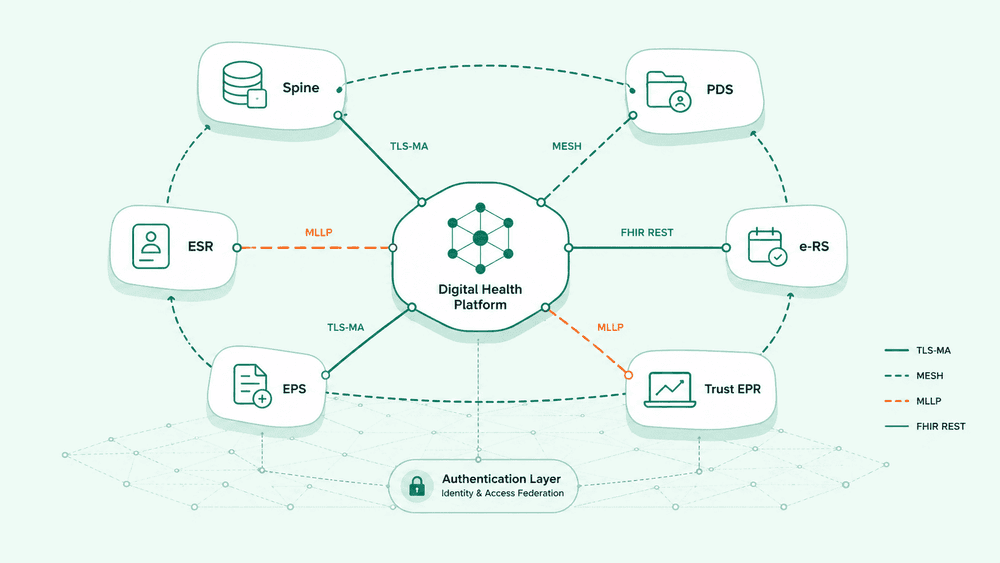
Spine is fronted by TLS Mutual Authentication, scoped to HSCN connectivity, with endpoint addresses that don't resolve from the public internet. PDS replies are structured but the trace pattern is multi-step, not a single lookup. e-RS and EPS are mediated by message exchange standards that long predate REST. HL7v2 ADT, ORU, and ORM messages still carry the bulk of intra-Trust integration traffic, often via TCP MLLP rather than HTTP. ESR exposes data through interfaces that were designed for batch and have been wrapped in newer surfaces without the underlying assumptions changing. FHIR R4 sits at the modern edge of all this, but the moment you cross from FHIR into a legacy estate, and you will, the model shifts again.
Healthcare API integration is the problem of moving structured clinical and demographic data across systems built across very different generations of design, under regulatory constraints that don't apply elsewhere, with patient safety implications when the data is wrong. It is not "more APIs."
The four NHS edges where naive REST design breaks
Once you start mapping a digital health platform onto the NHS estate, the same four edges break the same way every time.
1. Patient identity resolution is not a lookup.
Treating PDS as "GET /patient/{nhs_number}" misses how identity actually resolves in practice. A platform that doesn't have a verified NHS Number yet has to trace via demographics, handle multiple matches, deal with sensitive flags, and respect the smartcard or system-to-system access model that applies. Caching the response naively creates IG exposure. Not caching at all creates latency on every clinical screen. There is no clean middle ground without explicit design.
2. Asynchronous messaging is the default, not the exception.
MESH is the backbone for a large amount of NHS data movement, and it does not behave like a REST API. Messages are dropped into a mailbox, polled, acknowledged, and processed downstream. A platform whose integration logic assumes synchronous request and response will either build awkward polling loops on top, or worse, treat MESH as if it were HTTP and produce silent message loss when the mailbox state diverges from what the platform thinks happened.
3. Clinical safety creates write-side constraints REST doesn't anticipate.
DCB 0129 and DCB 0160 require clinical safety cases for the systems involved. That has direct API design consequences. Retries that are safe in an e-commerce flow can produce duplicate prescription orders or duplicated e-RS referrals if the integration doesn't manage idempotency at the clinical-event level rather than the HTTP level. Network timeouts that quietly retry can cause a single clinical action to land twice in a downstream system, and the consequence is no longer a duplicate order, it's a clinical incident.
4. The auth layer is many auth layers.
TLS Mutual Authentication for Spine, OAuth 2.0 for some FHIR APIs, NHS Care Identity (smartcard) for user-bound calls, NHSmail and Active Directory for staff identity, organisation-level credentials for system-to-system flows, and the Open API gateway model for newer services. A single platform integrating across the NHS estate is managing five or six authentication patterns concurrently. Treating auth as a generic concern is how teams ship configurations that pass dev and fail in production.
Each of these is a place where an integration designed on generic API thinking will hit a wall. The wall isn't visible during the build. It surfaces at month four, when scale, audit, or a Trust onboarding catches up.

Authentication is not an afterthought, it's an architecture decision
The single most under-budgeted area in healthcare API integration is authentication and credential management. NHS environments require, at minimum:
- TLS Mutual Authentication for Spine, with certificates that need to be rotated, monitored, and stored in line with NCSC guidance and DSPT expectations.
- Smartcard-mediated access for some clinical contexts, which constrains how user-acting flows can be built and how sessions are passed downstream.
- Per-organisation credentials for system-to-system flows, which scale poorly if treated as one credential per Trust without a managed rotation strategy.
- HSCN or modern equivalent network access for endpoints that don't resolve from the public internet.
A digital health platform that doesn't treat credential management as a first-class architecture concern ends up with secrets in environment variables, certificates that expire mid-pay-cycle, and an audit trail that can't answer the question "which environment used which cert when". The cost is invisible until the first expiry incident, after which it dominates roadmap conversations for a quarter.
The pattern that holds up is unglamorous: a managed credential vault scoped per environment, automated certificate lifecycle monitoring with alerting at 90, 30 and 7 days before expiry, an explicit registry of which auth pattern applies to which downstream system, and per-call audit logging that captures the credential identity used. None of this wins demos. All of it is what the difference between a platform that scales across Trusts and one that doesn't actually looks like.
The architecture pattern that holds up
The platforms that have stopped firefighting NHS integration tend to share five properties in their architecture.
They Separate the canonical model from the wire format.
HL7v2 on the wire, FHIR on the wire, and proprietary on the wire all map to the same internal canonical patient and event model. Transformations happen at the edge, not inside business logic. This is the single largest lever on long-term maintainability, and the one teams skip first when they're moving fast.
They Treat transport as plural.
The integration layer can speak HTTP/REST, MLLP, MESH, SFTP, and direct database where genuinely unavoidable. Treating one transport as the default and forcing others to fit it produces fragile adapters. Treating transport as a routing concern produces stable ones.
They Make idempotency explicit at the clinical-event level.
A referral, a prescription, an admission, and a result each have a natural identity. Integration logic deduplicates on those identities, not on HTTP request signatures. This is the difference between a safe retry and a clinical incident.
They Reconcile, don't assume.
Scheduled reconciliation jobs compare what was sent against what was received and surface variance for a human to investigate. The same pattern that prevents leave entitlement drift between ESR and rostering applies wherever two NHS systems hold what is meant to be the same data.
They Log at the field level, not the call level.
When a value is wrong, the question that always lands is "what did we send, what did we receive, what did we transform". A platform that can answer that question in seconds passes audit easily. A platform that can only answer at the request-id level spends weeks reconstructing each incident, and DSPT reviews become significantly more expensive than they need to be.
These five properties are not exotic. They are the difference between a healthcare API integration that survives contact with five Trusts and one that doesn't make it past three.
Where to start this quarter
If you are building or rebuilding a healthcare API integration layer right now, three steps are higher leverage than anything else.
- Inventory every downstream NHS system the platform touches and the auth pattern, transport, and message format each one uses. Most teams discover during this exercise that what they thought was three integration patterns is actually nine.
- Pick the canonical internal model the platform will hold patient and clinical-event data in, then write the explicit mapping to and from each external format. Resist the urge to use the wire format internally to "save time". You will pay it back with interest.
- Build the reconciliation job for the highest-volume integration point first. Even a daily diff between sent and received, ranked by variance, will surface issues that have been silently accumulating for months.
These are not glamorous architectural decisions. They are the ones that the senior IT Lead or Digital Lead inherits when the team that built the original integration has moved on, and the ones that determine whether the platform can scale beyond its first deployment.
The bottom line
Healthcare API integration in the NHS is not a harder version of normal API integration. It is a different problem with its own constraints, its own transport patterns, and its own audit expectations. The architectures that succeed are the ones designed for those constraints from day one.
If you are evaluating where your integration architecture sits today, the most useful single test is this: pick one downstream NHS system and ask whether your platform can answer, end to end, what was sent, what was received, what was transformed, and what is currently in flight. If the answer is yes, the rest of the pattern is achievable. If the answer is no, that is where the work starts this quarter.